

Umbilical hernia repair in adults
What it is, when it matters, and how it’s repaired
Mr Francesco Di Maggio · Last reviewed May 2026
An umbilical hernia is a soft lump at the navel that appears or grows because of a weak spot in the muscle wall. This guide is for adults who have noticed one and want to understand whether it should be repaired, what the operation involves, and what to expect afterwards.
What is an umbilical hernia?
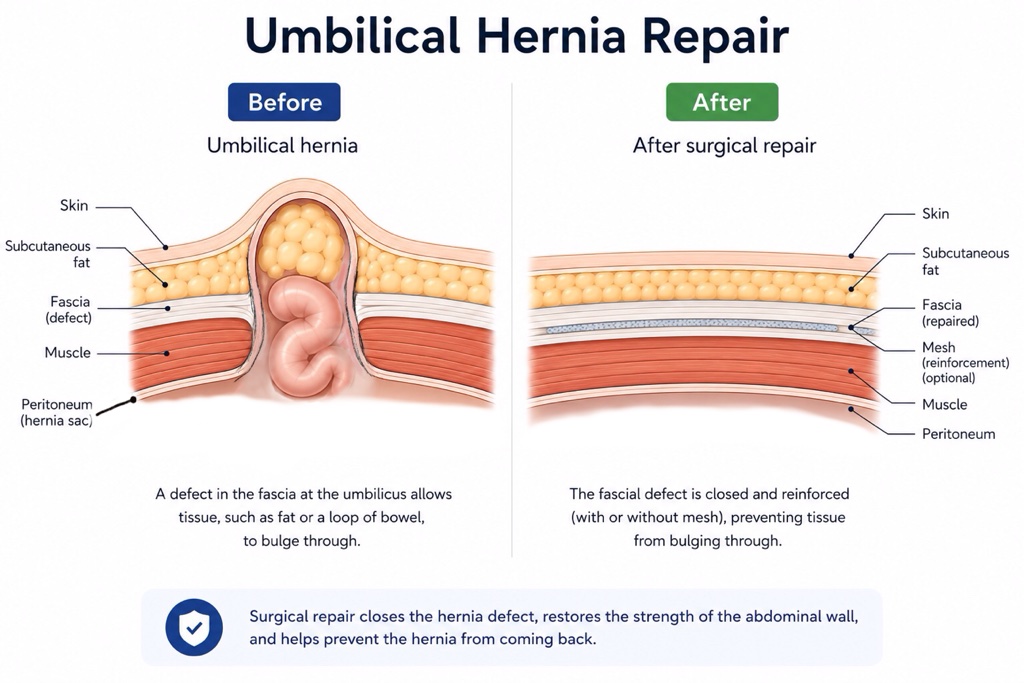
The abdominal wall is made of layers: skin, fat, then a sheet of strong fibrous tissue (fascia) and muscle, then a thin lining called the peritoneum. The fascia in the midline runs from the lower end of the breastbone down to the pubic bone. Where the umbilical cord came through at birth, that fascia is naturally a little thinner. In some adults the fascia gives way at that exact spot, leaving a small opening through which fat (and sometimes a loop of bowel) can push outward, creating a soft lump under the skin at the navel.
Umbilical hernias are common in adults. Many people will have one at some point in their lifetime, and many never produce symptoms or need treatment.
Umbilical hernias should not be confused with a separation of the rectus muscles down the midline (known as divarication or diastasis recti), which can look similar but does not contain herniated tissue. They are also distinct from epigastric hernias, which sit higher up the midline above the navel. A clinical examination usually distinguishes them; sometimes an ultrasound is helpful.
What causes one to develop?
Most adult umbilical hernias appear gradually, often after a period of raised pressure inside the abdomen. The main contributors are:
- Pregnancy and childbirth. The stretching of the abdominal wall during pregnancy is the single most common trigger in women, and hernias often appear or enlarge after multiple pregnancies.
- Obesity. A BMI consistently above 30 increases the load on the abdominal wall and weakens the fascia at the navel.
- Chronic cough, constipation, or heavy lifting. Persistent straining steadily widens any pre-existing weak spot.
- Liver disease with ascites. Free fluid in the abdomen exerts continuous pressure on the abdominal wall and is a common cause of larger umbilical hernias.
- Previous abdominal surgery. Operations performed through or near the umbilicus can leave a small weakness.
- Connective-tissue weakness. A small number of patients have an inherited tendency to hernias of various kinds, often in several family members.
Symptoms
Most umbilical hernias are noticed as a soft, sometimes painless bulge at the navel. The lump often gets larger when standing, coughing, or straining, and shrinks or disappears when lying down. That ability to “reduce” back into the abdomen is reassuring.
Common day-to-day symptoms include:
- A visible or palpable lump at the belly button.
- Discomfort or a dragging sensation, especially after eating, exercise, or a long day on your feet.
- A sharp, fleeting pain if the contents of the hernia briefly get pinched.
- Pressure marks from clothing, or thinned, shiny skin over a very large hernia that has been present for years.
When to seek urgent assessment
The following signs suggest the hernia may be incarcerated or strangulated, and need same-day medical attention or an A&E visit:
- A lump that has suddenly become hard, painful, and tender to the touch.
- A tender lump you cannot push back in when you have always been able to before.
- Nausea, vomiting, or inability to pass wind or stool, especially when accompanied by abdominal pain.
- Skin over the lump turning red, dusky, or unusually warm.
These are uncommon but serious. Repair of a strangulated hernia is a much bigger undertaking than a planned operation, and outcomes are better when patients are seen early.
When does it need surgery?
Two situations call for repair without much debate. The first is when the hernia is producing real symptoms, such as pain, restriction of activity, or interference with clothing. The second is when there is a meaningful risk of complications.
Small, soft, painless umbilical hernias in patients who are otherwise well can often be watched. But once a hernia is symptomatic, or once it is enlarging quickly, repair is generally the safer long-term option than waiting for an emergency. Emergency repair carries a higher rate of complications and a longer recovery than a planned operation.
Decisions are more nuanced in particular groups:
- Patients with significant liver disease and ascites. Repair is often deferred until the fluid is controlled, because operating in the presence of uncontrolled ascites raises the risk of wound complications and recurrence.
- Women planning further pregnancy. Repair is often best timed after the family is complete, since pregnancy can stretch the repair and bring the hernia back.
- Patients with high BMI. Weight loss before surgery (even modest) measurably reduces the risk of recurrence and wound complications.
How the operation works
Umbilical hernia repair is one of the most commonly performed operations in general surgery. It is almost always done as a day case and takes between 30 minutes and an hour for an uncomplicated case. For recurrent or larger hernias, it can take longer.
Most repairs are performed under general anaesthesia. For small primary defects in patients who prefer to avoid a general anaesthetic, a repair under local anaesthesia (with or without sedation) is sometimes possible.
There are two main surgical approaches:
- Open repair uses a small incision in the crease of the umbilicus. The contents are pushed back, the fascial defect is closed with strong sutures, and (for all but the smallest hernias) a piece of synthetic mesh is positioned underneath the fascia to reinforce the repair. Without mesh, recurrence rates are high for any hernia bigger than around one centimetre, which is why current European Hernia Society guidance recommends mesh for almost all adult umbilical hernias.
- Laparoscopic (keyhole) repair uses three small ports placed away from the umbilicus. The defect is repaired from inside the abdomen and a sheet of mesh is fixed underneath. Keyhole repair can be used for recurrent hernias, and patients who have several small defects along the midline at once.
The choice between open and laparoscopic depends on the size of the defect, what is inside the hernia, your previous surgical history, and your preference. Both produce good results in experienced hands.
Recovery and what to expect
Most patients go home the same day. Pain is moderate for the first two or three days and is well controlled with simple painkillers (paracetamol with a short course of ibuprofen, occasionally a stronger painkiller in the first 24–48 hours).
Practical guidance for the first few weeks:
- Lifting: avoid lifting anything heavier than a kettle for two weeks; build back to normal lifting over four to six weeks.
- Driving: usually safe after one to two weeks, once you can perform an emergency stop without hesitation. Check also with your motor insurer.
- Work: desk-based work can usually be resumed within three to seven days. Physical work typically needs two to four weeks off.
- Exercise: walking is encouraged from day one; gentle aerobic exercise after two weeks; resistance training and core work from four to six weeks.
- Showering is fine after 48 hours; baths and swimming after the wound has fully healed at around two/three weeks.
- Sex can be resumed as soon as it feels comfortable, usually within a week or two.
There is some bruising around the wound for a fortnight, and a firm “ridge” where the mesh sits is normal: both settle over six to eight weeks. The umbilicus often looks subtly different afterwards, especially after repair of a larger hernia. Some numbness around the scar is normal and tends to improve over months.
Outcomes
Recurrence rates after mesh repair of a typical adult umbilical hernia are around 5% at five years. Without mesh, recurrence rates for hernias larger than around two cm run substantially higher. Other measures (wound healing, return to work, patient-reported satisfaction) are uniformly high in modern series.
Risks
The risks of an uncomplicated umbilical hernia repair are low but not zero:
- Recurrence: around 5% with mesh repair, considerably higher without it, or in patients with high BMI and smokers.
- Wound infection: uncommon, more frequent in patients with diabetes or who smoke.
- Seroma (fluid collection under the skin): usually settles on its own; very occasionally needs drainage.
- Discomfort or numbness around the scar, usually mild and time-limited.
- Cosmetic change in the appearance of the umbilicus, particularly after repair of larger hernias.
- Mesh-related complications: infection, chronic discomfort, or, very rarely, erosion. Together these affect well under 1% of patients.
- Standard general-surgery risks: bleeding, anaesthetic risks, blood clots in the legs or lungs.
- Conversion of a laparoscopic operation to open surgery: uncommon, but recommended if it makes the operation safer.
When to seek a consultation
If you have a lump at the navel that hurts, has grown over time, or has ever become hard, tender, or impossible to push back in, you should be seen. Bring a list of your medications, your weight and height, and any imaging that has already been done. Most umbilical hernias can be repaired definitively in a single day-case operation.
Frequently asked questions
Will an umbilical hernia get worse if I leave it?
Most do enlarge gradually over years, especially with weight gain, pregnancy, or heavy lifting. Larger hernias are technically harder to repair and have higher recurrence rates than small ones, both reasons to consider repair sooner rather than later once symptoms appear.
Can I exercise with an umbilical hernia?
Generally yes. Exercise does not cause hernias, and continuing to exercise will not make the hernia bigger any faster than ordinary daily activity. Very heavy lifting and high-impact activity however can cause discomfort or contribute to making the hernia larger. Core work (sit-ups, plank variations) sometimes brings on symptoms.
Will I have a scar?
Yes. For small hernias, it can be tucked into the natural folds of the umbilicus and is hard to see after a few months. For larger hernias, it will be visible above the umbilicus. Laparoscopic repair leaves three very small scars well away from the navel itself.
Is mesh safe?
Modern synthetic mesh has been used in millions of hernia repairs and has a strong safety record. The risk of mesh-related complications (infection, chronic discomfort) is low and well-studied. The benefit (a much lower recurrence rate) almost always outweighs the risk in adult umbilical hernias bigger than around 1.5 centimetre.
Can I still have children after umbilical hernia repair?
Yes. Pregnancy after a mesh repair is safe for both mother and baby. However, the stretching of the abdominal wall during pregnancy increases the chance of the repair failing and hernia coming back, so women planning further children are often advised to delay surgery until the family is complete.
What if I have other lumps along the midline?
You may have more than one hernia at the same time. For example, a small umbilical hernia and a small hernia just above the navel (an epigastric hernia) is a common combination. They can usually be repaired together in one operation. Your surgeon will examine you carefully and explain what they find.
How soon can I fly after the operation?
Short-haul flights are usually fine after two weeks. Long-haul travel is better delayed for at least three weeks, mostly because of the higher risk of blood clots in the legs after any operation. Luggage handling and lifting is not recommended for up to six weeks.
Book a consultation with Mr Di Maggio
Consultations are available at New Victoria Hospital (Kingston), Dottore London (Holborn), St Anthony’s Hospital (Sutton) and Shirley Oaks Hospital (Croydon). Bring any recent scans, endoscopy reports, and a list of your current medications.