

Paraesophageal hernia repair
The hiatus hernia most patients have never heard of
Mr Francesco Di Maggio · Last reviewed May 2026
Paraesophageal hernia is the less common (and often more serious) type of hiatus hernia. This guide explains what it is, how it’s different from the sliding hernia most people are familiar with, when it needs to be repaired, and what to expect from surgery.
What is a paraesophageal hernia?
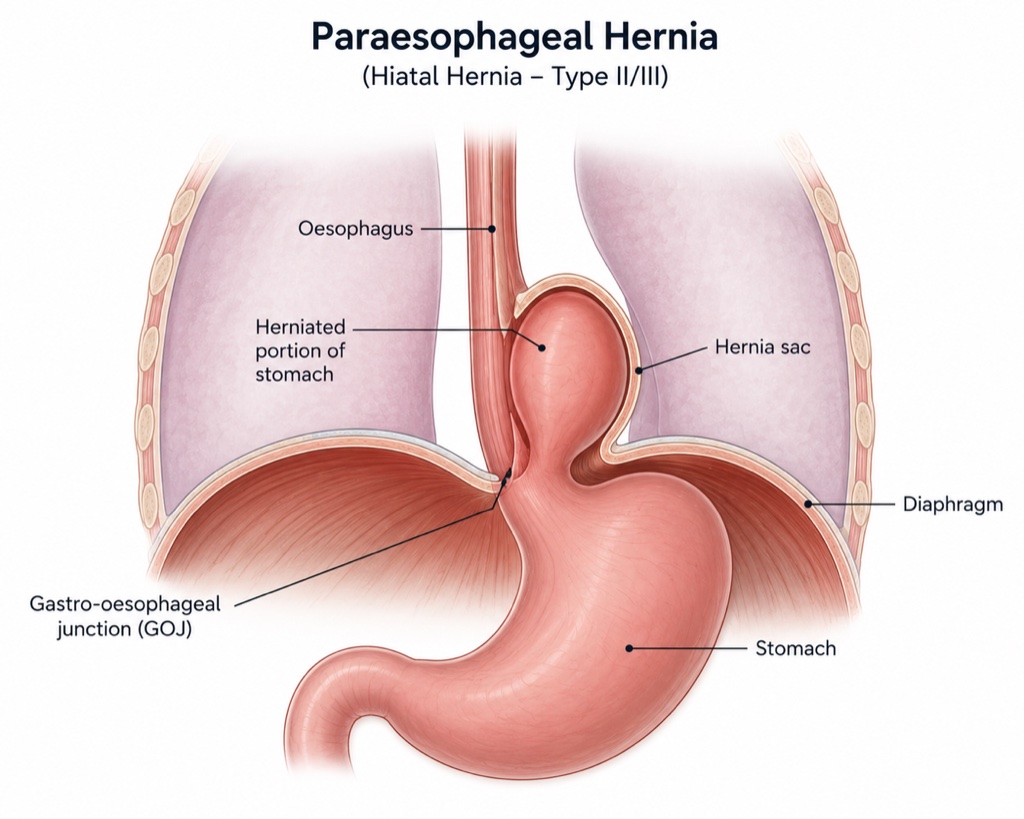
The diaphragm is the broad sheet of muscle that separates the chest from the abdomen. The food pipe (oesophagus) passes through a small opening in the diaphragm called the hiatus before joining the stomach just below it. In a hiatus hernia, part of the stomach pushes upward through this opening into the chest.
Most patients have heard of the common form, the sliding hiatus hernia, in which the junction between the oesophagus and stomach slides up into the chest and back down again with breathing and posture. This is the type most commonly associated with reflux disease, and it can be managed with medication, lifestyle measures, or surgery.
A paraesophageal hernia is different and less common. Here, the junction between the oesophagus and stomach is not the part that herniates. Instead, the upper part of the stomach (the fundus) pushes upward alongside the oesophagus through a widened gap in the diaphragm. As the hernia enlarges, more of the stomach (and, in very advanced cases, other organs such as the colon or spleen), can migrate into the chest.
The four types of hiatus hernia
Surgeons classify these on anatomical grounds:
- Type I: sliding hernia (the common type).
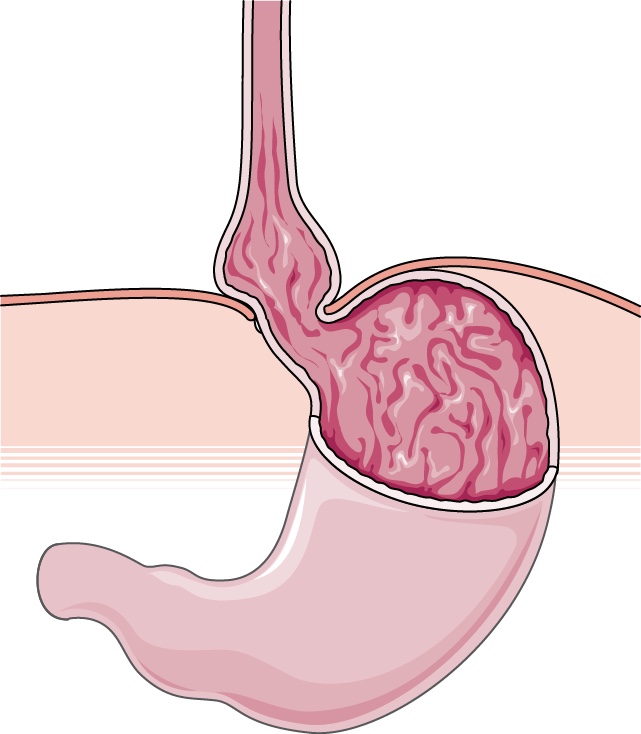
- Type II: true paraesophageal hernia: the oesophago-gastric junction stays below the diaphragm, only the fundus herniates upward (rare).
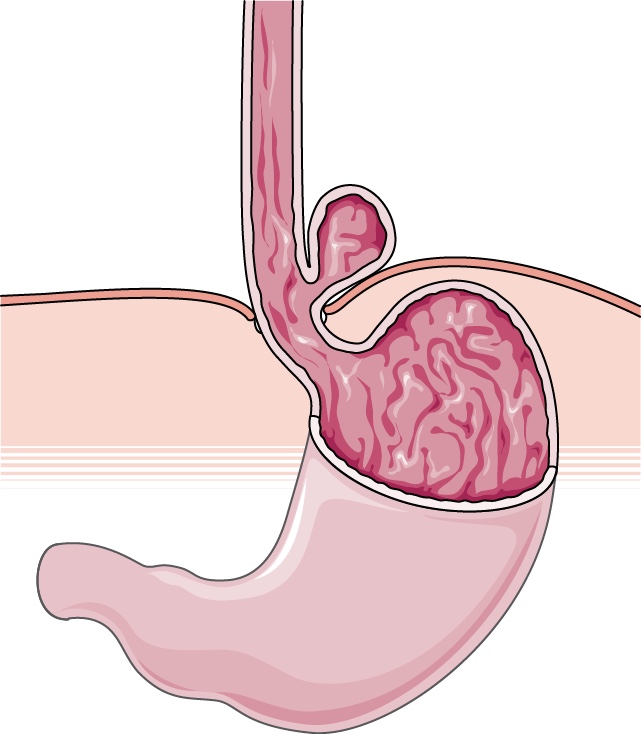
- Type III: mixed hernia: both the junction and a portion of the stomach migrate upward (the most common paraesophageal form).
- Type IV: additional organs (colon, spleen, pancreas, or omentum) migrate into the chest alongside the stomach.
Together, paraesophageal hernias (Types II–IV) account for roughly 5–15% of all hiatus hernias.
What causes one to develop?
Most paraesophageal hernias appear gradually, over years, in patients in the second half of life. Several factors contribute:
- Age — most patients are over 60 by the time the hernia becomes significant.
- Persistent raised intra-abdominal pressure: obesity, chronic cough, heavy lifting, long-standing constipation.
- Connective-tissue weakness in the diaphragmatic hiatus.
- Previous anti-reflux or upper-abdominal surgery.
- Individual predisposition including spinal deformities.
Symptoms — what to look out for
Paraesophageal hernias often produce a different pattern of symptoms from a typical sliding hiatus hernia. Heartburn may be absent or only mild. Instead, patients commonly describe:
- A sense of fullness or pressure in the chest after eating, sometimes mistaken for a heart symptom.
- Difficulty swallowing, or food sticking briefly after meals.
- Recurrent chest pain or breathlessness on exertion — the stomach sitting in the chest can compress the lungs.
- Inability to lay flat due to significant reflux of gastric content.
- Unexplained iron-deficiency anaemia, caused by slow oozing from a stretched, congested stomach lining.
- Episodes of vomiting that bring up undigested food, sometimes long after eating.
In a small number of patients, the herniated stomach can twist on itself — a condition called gastric volvulus. This is a life-threatening surgical emergency. It produces severe chest or upper-abdominal pain, retching without being able to vomit, and an inability to swallow even saliva. It needs immediate hospital assessment.
When is surgery recommended?
The decision is individual and depends on three things: how large the hernia is, what symptoms it is causing, and the patient’s overall health.
Surgery is strongly recommended if a paraesophageal hernia has caused a complication such as bleeding, obstruction, or volvulus, or if it is making normal eating or sleeping difficult. Larger, symptomatic hernias are also best repaired electively, before a complication forces an emergency operation. Asymptomatic or minimally symptomatic hernias in older or frailer patients can sometimes be watched safely.
International guidance has moved away from operating on every paraesophageal hernia simply because it is present. The decision is made jointly with the patient after a careful conversation about benefits, risks, and personal circumstances.
How the operation works
Repair is almost always carried out laparoscopically (keyhole), through four or five small ports in the upper abdomen. Open surgery is rarely necessary in modern practice.
The operation has three core steps:
- Reduction of the hernia sac and its content. The hernia sac is carefully dissected away from the lung, heart, and great vessels in the chest, which is the most technically demanding part of the operation. The herniated stomach (and any other organs in the chest) is gently brought back down into the abdomen.
- Closure of the hiatus. The widened gap in the diaphragm is closed with strong sutures. For larger defects, the repair may be reinforced with a small piece of mesh (biological or absorbable synthetic) to reduce the risk of recurrence.
- Anti-reflux procedure. A fundoplication (partial or full wrap of the upper stomach around the lower oesophagus) can be added. This serves two purposes: it reduces post-operative reflux, and it anchors the stomach below the diaphragm so it cannot slide back up.
The operation typically takes between two and three hours under general anaesthesia. Most patients stay in hospital for one or two nights. However, the larger the hernia, the longer the operation (and the recovery) will take.
Recovery and what to expect
For the first four weeks the diet is restricted to soft foods. Patients are advised to eat slowly, chew thoroughly, and avoid bread, dry meat, and bulky vegetables. Carbonated drinks are best avoided in the first month. Normal food is reintroduced gradually over four to six weeks.
Most patients are back to desk work within two weeks and to physical work, or vigorous exercise, within four to six weeks.
Some early symptoms are expected and settle on their own:
- Difficulty bringing up wind, with a sense of trapped gas.
- A feeling that the stomach is full after only a few mouthfuls.
- Inability to vomit during the first few weeks.
These typically ease over the first weeks as the swelling at the hiatus settles and the new anatomy beds in.
Outcomes
Roughly 85–90% of patients have good or excellent symptom control five to ten years after a well-performed elective paraesophageal hernia repair. Most patients who have a small recurrence on follow-up imaging are not aware of it and do not need re-operation.
Risks
Like any major operation, paraesophageal hernia repair carries risks. The important ones to be aware of are:
- Recurrence of the hernia (the most common long-term issue), occurring in around 10–15% of patients over ten years. Most recurrences are small and do not require re-operation.
- Difficulty swallowing in the first few weeks, usually temporary.
- Bloating or excess wind (so-called gas-bloat syndrome), more common after a full wrap and usually settling over months.
- Flatulence or diarrhoea in the first few weeks.
- Damage to nearby structures (the spleen, liver, oesophagus, or vagus nerves), rare in experienced hands.
- Standard general-surgery risks: bleeding, wound infection, blood clots in the legs or lungs, chest infection.
- Mortality is very low for elective repair, in the order of 0.5% or less, depending largely on the patient’s overall health and the urgency of the operation.
When to seek a consultation
If you have been diagnosed with a paraesophageal hernia, or if you have any of the symptoms above and want to understand whether your hernia is the type that needs repair, a consultation is the right next step. Bring any recent gastroscopy, barium swallow, or CT reports — they save time and avoid duplicating tests.
Frequently asked questions
How is a paraesophageal hernia diagnosed?
Most are first picked up on a gastroscopy (camera test) or a CT scan of the chest and abdomen performed for unrelated reasons. A barium swallow is sometimes added to show how the stomach moves dynamically. Before surgery, oesophageal manometry and a 24-hour pH study are usually arranged to plan the most appropriate type of anti-reflux procedure.
Is a paraesophageal hernia dangerous?
Most paraesophageal hernias are not immediately life-threatening, but they can cause troublesome symptoms and tend to enlarge slowly over time. The serious complication (gastric volvulus) is rare, but it is a true life-threatening emergency. This is why symptomatic hernias are generally repaired before a complication develops.
Can it be treated without surgery?
Acid-related symptoms can often be controlled with proton-pump inhibitors, and weight loss or better control of a chronic cough can reduce day-to-day pressure on the diaphragm. But medication and lifestyle measures do not change the anatomy. If the hernia is causing chest pressure, swallowing difficulty, or bleeding, surgery is the only definitive treatment.
How long does the operation take?
Typically within three hours under general anaesthesia for an uncomplicated case. Larger or recurrent hernias can take longer.
When can I drive after surgery?
Usually after two weeks, once you can comfortably perform an emergency stop without hesitation. Check with your motor insurer.
Book a consultation with Mr Di Maggio
Consultations are available at New Victoria Hospital (Kingston), Dottore London (Holborn), St Anthony’s Hospital (Sutton) and Shirley Oaks Hospital (Croydon). Bring any recent scans, endoscopy reports, and a list of your current medications.