

Laparoscopic Anti-Reflux Surgery (Nissen Fundoplication)
Published: 30/03/2025
A safe and effective surgery to reduce symptoms of reflux, reliance on medications, and improve quality of life.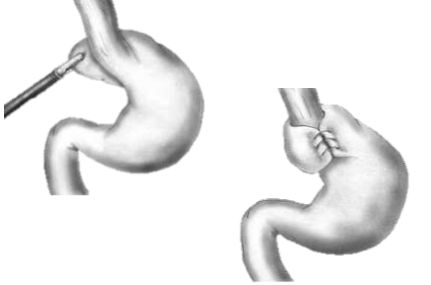
Up to 20% of adults in the UK suffer from reflux disease, often referred to as GORD (Gastro-Oesophageal Reflux Disease).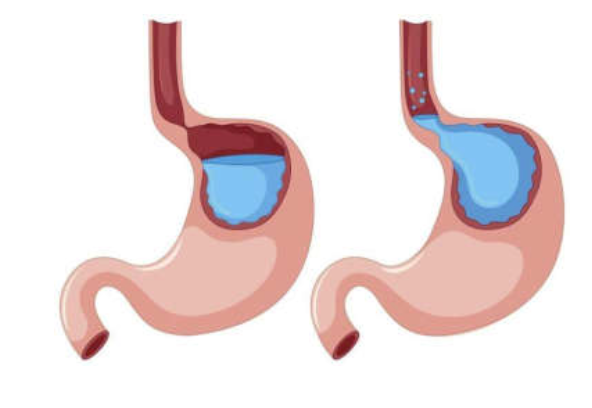
 An ineffective sphincter at the bottom of the oesophagus is often found to be the cause. However, many adults also have a small part of their stomach herniating into the lower part of the chest, through the diaphragm.
An ineffective sphincter at the bottom of the oesophagus is often found to be the cause. However, many adults also have a small part of their stomach herniating into the lower part of the chest, through the diaphragm.
A gap in the diaphragm (known as the oesophageal hiatus) provides support to the sphincter as the oesophagus passes from the chest into the abdomen.
If the stomach is pushing up through this gap, the support is lost, and acid can easily flow up the oesophagus.
In the most severe cases, the portion of the stomach herniating into the chest will increase with time. More of the stomach will push against the lungs, causing worsening respiratory symptoms.
Exceptionally, patients can develop life-threatening complications from this condition, such as stomach volvulus (when the stomach twists on its axis into the chest), requiring emergency life-saving operations.
In most cases, the operation is performed with keyhole (laparoscopically), through four or five small cuts in the abdomen.
Any hiatus hernia is pulled back into the abdomen, and the hiatus is tightened using stitches. To reinforce the sphincter, the upper part of the stomach (fundus) is wrapped around the lower oesophagus and stitched together as in the below diagram.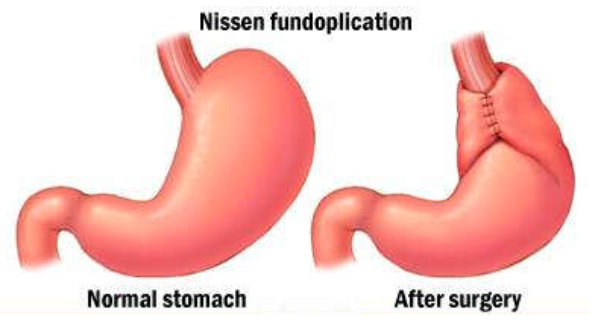
 Laparoscopic anti-reflux surgery involves the use of a camera and keyhole instruments, which pass through four/five small holes in the abdomen. You will be asleep for the entire procedure.
Laparoscopic anti-reflux surgery involves the use of a camera and keyhole instruments, which pass through four/five small holes in the abdomen. You will be asleep for the entire procedure.
From then, you should not do any heavy lifting or strenuous exercise for 4-6 weeks.
Depending on what you do for work, you will go back after 3-4 weeks. You will be followed up in an outpatient clinic after approximately 3 months, with a further follow-up after another 3 months if necessary.
You will be started on a soft diet post-operatively, with gradual introduction of solid food, in the 6 weeks following your operation.
What is reflux?
Acid reflux is the result of acid in the stomach coming up into the oesophagus (food pipe) which should be naturally acid-free. Normally, the lower oesophageal sphincter and the anatomy of the gastro-oesophageal junction would prevent this.Up to 20% of adults in the UK suffer from reflux disease, often referred to as GORD (Gastro-Oesophageal Reflux Disease).
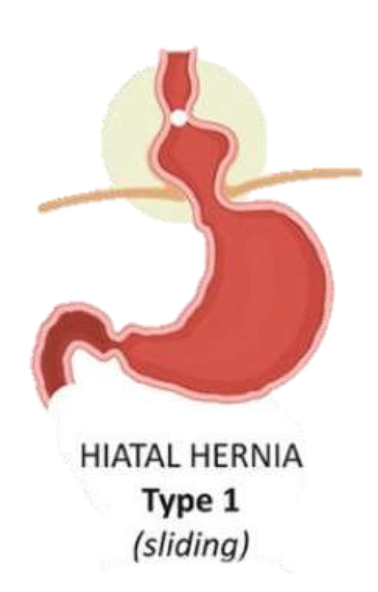
What causes reflux?
An ineffective sphincter at the bottom of the oesophagus is often found to be the cause. However, many adults also have a small part of their stomach herniating into the lower part of the chest, through the diaphragm.A gap in the diaphragm (known as the oesophageal hiatus) provides support to the sphincter as the oesophagus passes from the chest into the abdomen.
If the stomach is pushing up through this gap, the support is lost, and acid can easily flow up the oesophagus.
In the most severe cases, the portion of the stomach herniating into the chest will increase with time. More of the stomach will push against the lungs, causing worsening respiratory symptoms.
Exceptionally, patients can develop life-threatening complications from this condition, such as stomach volvulus (when the stomach twists on its axis into the chest), requiring emergency life-saving operations.
Is reflux a problem?
Many people have reflux but do not have any symptoms. Often though, acid reflux is incredibly uncomfortable and impacts daily life. Patients with GORD might develop:- Burning in their chest or throat
- Chest pain
- Regurgitation when stooping or straining
- Reduced tolerance to exercise
- Poor quality sleep due to reflux when lying flat.
How to treat reflux?
- In the first instance, patients are advised to change their diet and adopt a few useful habits, such as reducing the size of their meals, not eating too close to bedtime, and avoiding sparkling beverages, caffeine, alcohol, and fried food.
- The next step would be starting some medications, such as Omeprazole or Famotidine, which reduce acid production or tamponade the acid in the stomach.
- For patients who heavily rely on these medications to keep their symptoms under control, patients who experience side effects from them, and patients who still experience GORD symptoms despite the medications, anti-reflux surgery should be considered.
Anti-reflux surgery
In the UK, the most commonly performed operation to treat reflux is a Nissen Fundoplication.In most cases, the operation is performed with keyhole (laparoscopically), through four or five small cuts in the abdomen.
Any hiatus hernia is pulled back into the abdomen, and the hiatus is tightened using stitches. To reinforce the sphincter, the upper part of the stomach (fundus) is wrapped around the lower oesophagus and stitched together as in the below diagram.
Benefits and alternatives
The main benefit of having this operation is to improve GORD symptoms, such as reflux, heartburn, and chest pain, without the need to rely on medication.The Operation
Laparoscopic anti-reflux surgery involves the use of a camera and keyhole instruments, which pass through four/five small holes in the abdomen. You will be asleep for the entire procedure.- The top part of the stomach (fundus) and the lower oesophagus are carefully freed from their nearby structures;
- The hiatus is repaired and made tighter;
- The newly freed fundus is wrapped around the lower oesophagus, either 270° (Toupet fundoplication) or 360° (Nissen fundoplication), to reinforce the sphincter and reconstitute an anti-reflux barrier;
- You will then remain in hospital for some days, and once your post-operative pain is under control, you mobilise and are able to tolerate a liquid diet, you will be discharged home.
After Surgery
After 2-3 days, you should be fit to be discharged home.From then, you should not do any heavy lifting or strenuous exercise for 4-6 weeks.
Depending on what you do for work, you will go back after 3-4 weeks. You will be followed up in an outpatient clinic after approximately 3 months, with a further follow-up after another 3 months if necessary.
You will be started on a soft diet post-operatively, with gradual introduction of solid food, in the 6 weeks following your operation.